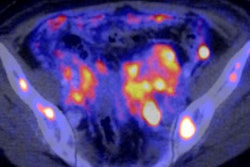
While PET/MRI shows great promise in a multitude of clinical applications, German researchers have found that the hybrid modality's performance in evaluating head and neck cancer appears no better than that of tried-and-true PET/CT.
There were no statistically significant differences between FDG-PET/MRI and FDG-PET/CT for diagnosing head and neck cancer, said lead author Dr. Benedikt Michael Schaarschmidt from the University of Düsseldorf, who presented study results at RSNA 2016 in Chicago.
"We can conclude that although PET/MRI gives us improved soft-tissue contrast in the head and neck, the accuracy for head and neck tracer uptake is not better than PET/CT," Schaarschmidt said. "Therefore, [PET/MRI] does not improve diagnostic accuracy."
Incidental uptake
Head and neck cancer is one clinical application that has benefited from PET/CT since the technology's inception some 15 years ago. However, when using hybrid modalities such as PET/CT and PET/MRI, clinicians frequently observe incidental tracer uptake in the course of their diagnoses.
"Although some of this incidental tracer uptake is quite easy to diagnose, diagnostic tests are sometimes necessary" to confirm the results, Schaarschmidt said. "This is quite problematic for the patient, especially if you have to perform a biopsy that may even be harmful."
Thus, the researchers sought to answer three questions:
- Does the enhanced soft-tissue contrast of PET/MRI offer additional information in the head and neck area, compared with PET/CT?
- Does PET/MRI improve sensitivity in incidental tracer uptake?
- Do these results affect FDG-PET/MRI's diagnostic accuracy?
Schaarschmidt and colleagues performed a retrospective analysis of 81 patients who underwent PET/CT and subsequent PET/MRI scans with a commercially available system (Biograph mMR, Siemens Healthineers) on the same day. The PET/CT protocol included a dedicated contrast-enhanced head and neck scan, while the PET/MRI protocol included both noncontrast and contrast-enhanced MR sequences.
Two independent readers interpreted the fused PET/CT and PET/MR datasets in random order on two separate sessions for PET/CT and PET/MRI studies. Tracer uptake was characterized as most likely malignant, indeterminate, or most likely benign.
As a reference standard, findings were classified as benign or malignant based on all radiological, histopathological, and clinical examinations. To assess accuracy, indeterminate findings were deemed to be inaccurate results. A p-value of less than 0.05 was considered statistically significant.
Lesion count
A total of 46 lesions were available for further analysis. Based on the reference standard, 43 lesions were benign and one lesion was malignant. A definitive diagnosis was not possible in two cases.
While PET/CT and PET/MRI each correctly classified incidental tracer uptake in 28 cases, 14 results were incorrectly classified by either modality. In addition, four findings misclassified on PET/CT were correctly identified by PET/MRI.
The researchers found no statistically significant differences in terms of characterizing the lesions as malignant, benign, or indeterminate. PET/MR was not superior to PET/CT regarding the correct diagnosis of incidental FDG uptake (p = 0.125).
| PET/CT, PET/MRI in head and neck cancer | |||
| Modality | Lesion type | ||
| Benign | Indeterminate | Malignant | |
| PET/CT | 27 | 18 | 1 |
| PET/MRI | 31 | 14 | 1 |
Schaarschmidt and colleagues attributed the lack of a statistically significant difference in MRI's soft-tissue contrast ability as the reason why the modality did not provide any additional relevant information for a correct diagnosis.
When asked whether adding diffusion-weighted MRI (DWI-MRI) might advance head and neck cancer evaluation and diagnosis, Schaarschmidt told RSNA attendees that he has known of dozens of cases in which DWI did not contribute any additional information.
He cited one case in which a patient showed a small difference in tracer uptake in the tonsils, but DWI did not reveal anything. The patient eventually underwent biopsy, and clinicians found a T1 tonsillar cancer.
"I think diffusion-weighted imaging might be helpful in selected cases, but in my opinion, I always put the PET first," Schaarschmidt said. "If the PET [result] is obvious, I always believe the PET and ... I think diffusion-weighted imaging is a little overestimated in the head and neck."