Computer-aided detection (CAD) enhances the ability to pinpoint hard-to-find flat colorectal lesions in CT colonography (CTC) -- for all but the very best readers, that is, Italian researchers have found.
 Dr. Mariangela Santoni from the University of Rome La Sapienza.
Dr. Mariangela Santoni from the University of Rome La Sapienza.Radiologists from the University of Rome La Sapienza used CAD as a second reader on about 200 CTC patients -- half negative and half with nonpolypoid, or flat, lesions. The images were interpreted by radiologists at four different experience levels from novice to expert. Detection sensitivity rose by as much as 10% for less-experienced readers with the use of CAD, but did not rise significantly when an expert reader used the tool.
"In all test results, the detection rate of expert readers gained only a small increase using CAD as a second reader," said Dr. Mariangela Santoni in a presentation at ECR 2016. "On the other hand, we observed that intermediate and novice radiologists may see higher sensitivity using the CAD versus the non-CAD technique."
Flat lesions: Rare or not?
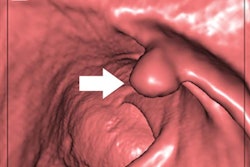
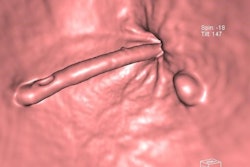
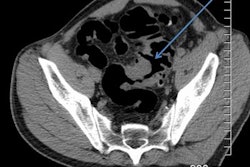
Taking aim at a tough detection problem, the researchers set out to evaluate the utility of computer-aided detection in "this difficult finding," Santoni said. Nonpolypoid or flat lesions are 2.5 mm or less in height, and can be slightly depressed, completely flat, or slightly elevated, she said. Detection of such lesions has presented a perennial challenge for CT colonography as well as the conventional kind.
The literature reports a prevalence of 5% to 50% for such lesions, a very wide range that "may be due to a lack of assessment of diagnostic criteria," she said. Also, many radiologists and endoscopists lack experience in diagnosing these lesions, resulting in more missed detections.
Finally, many optical colonoscopy centers lack high-definition white-light endoscopy systems and chromoendoscopy systems that ensure optimal evaluation of nonpolypoid lesions, and the possibility of misclassifying slightly elevated lesions of the sessile and polypoid subtypes is substantial, Santoni said.
Controls and flat polyps
"We are evaluating the usefulness of CAD as a second reader according to the different levels of experience of radiologists," she said.
The study authors anonymized and randomly reviewed 94 patients with nonpolypoid lesions (108 in all) and 100 patients as a control group, whose results were negative both at CTC and optical colonoscopy.
Bowel prep began with a low-residue diet followed by polyethylene glycol and iodinated oral contrast. Distention was performed by manual air insufflation. CT colonography data were acquired on a 64-detector-row scanner.
The results were first by 2D/3D CTC by four radiologists with different experience levels who were blinded to the results. The four readers included an expert (> 5,000 exams), an intermediate reader (50 to 300 exams) and two novice radiologists (< 50 cases each).
Also measured were the positive predictive value (PPV), the false-positive rate, and reporting time for individual readers, Santoni said. One month later, all images were reanalyzed using the 2D/3D technique plus CAD (im3D, Medical Imaging Lab) as a second reader.
All positive patients underwent optical colonoscopy and biopsy, and the group performed statistical analysis to calculate inter-reader agreement.
Several measures show improvement with CAD
The expert reader saw a trend toward higher sensitivity but no statistically significant improvement with CAD, while the intermediate and novice readers all saw statistically significant improvement with the use of CAD, Santoni said.
Sensitivity improved significantly only for intermediate and novice readers with the addition of CAD.
| Reader | Sensitivity: 2D-3D interpretation | Sensitivity: 2D-3D plus CAD | P value |
| Expert | 74% | 84% | p = 0.066 |
| Intermediate | 65% | 78% | p = 0.0033 |
| Novice 1 | 50.9% | 69% | p = 0.008 |
| Novice 2 | 57% | 72% | p = 0.0022 |
CAD increased the PPV for novices more than for experts.
| Reader | Sensitivity: 2D-3D interpretation | Sensitivity: 2D-3D plus CAD | Increase in PPV |
| Expert | 0.89 | 0395 | 0.06% |
| Intermediate | 0.77 | 0.85 | 0.08% |
| Novice 1 | 0.61 | 0.78 | 0.17% |
| Novice 2 | 0.61 | 0.77 | 0.16% |
"Reporting time demonstrated a small increase using CAD, but the increase in reporting time wasn't statistically significant at all experience levels of radiologists," she said.
Trend toward fewer false positives with CAD
Moreover, false positives actually decreased with the addition of CAD, from nine to four for the expert reader, from 20 down to 14 with the intermediate reader, and from 35 to 20 for the first novice reader, Santoni reported.
"CAD improves the detection rate of nonpolypoid lesions, especially in intermediate and novice readers," she said. In addition, there was no statistically significant increase in reporting time, and CAD offered a low false-positive rate.