Iterative reconstruction is fast becoming the magic bullet for CT dose reduction, but if you have an older CT scanner without this function, what can you do? Adjusting the scanning range of CT pulmonary angiography cuts dose by 24% and is safe, with a low recall rate, U.K. researchers have reported.
Across Europe, the number of CT pulmonary angiograms being performed is increasing year on year, yet the positivity rate is decreasing, and in some studies it has dropped from 20% to 5%, according to Dr. Rute Martins, radiology registrar at Portsmouth Hospitals National Health Service (NHS) Trust. Therefore, more patients are being exposed to medical radiation, putting an ever-greater emphasis on the implementation of measures designed to reduce CT radiation dose.
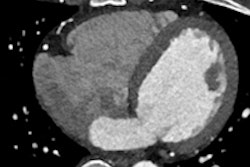
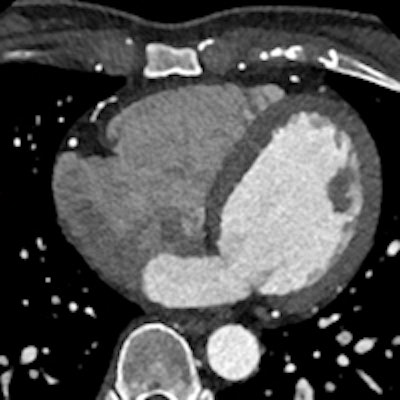
 If you have it, iterative reconstruction can be an effective way to reduce dose. This 0.2-mSv cardiac CT angiography examination demonstrates standard reconstruction versus iterative model reconstruction (IMR). Image courtesy of Philips Healthcare.
If you have it, iterative reconstruction can be an effective way to reduce dose. This 0.2-mSv cardiac CT angiography examination demonstrates standard reconstruction versus iterative model reconstruction (IMR). Image courtesy of Philips Healthcare.In hospitals where iterative reconstruction is not available, other methods can be employed, she informed delegates in an e-poster at the 2015 annual meeting of the European Society of Thoracic Imaging (ESTI), held in Barcelona, Spain.
Research has shown that reducing the peak voltage (kVp) of CT pulmonary angiography from 120 to 100 cuts dose by 33%, she explained. Gravity causes lung perfusion to be better at the base than at the apex, and as such, there is a relative scarcity of pulmonary vessels within the apices. This simple fact about the organization of pulmonary circulation will then translate into the low probability of diagnosis of thromboembolism uniquely at the level of the apices; conversely, it is at the level of the apices that the radiation dose is higher due to the overlying structures, i.e., skeletal, she added.
Study design and results
Martins and her colleagues designed a study to assess the safety and efficacy of radiation dose reduction in hospitals lacking iterative reconstruction. The retrospective study of their current CT pulmonary angiography practice focused on reducing the z axis by scanning from the aortic arch to the lung bases, and was undertaken to determine the dose reduction and recall rate.
A total of 200 consecutive patients underwent CT pulmonary angiography between March and May 2014, prior to a change in protocol. The entire lung field was scanned in this control group. A further 200 consecutive patients who were scanned using the new reduced z axis protocol were selected from August to November 2014.
Details of these patients were recorded to include age, dose length product (DLP), scan kVp, scan findings, and recall rate. The average age of the selected population was 66. Overall, 2% of the scans of the total number of patients were positive for thromboembolism. A total of 99% of patients in both the control and subject groups were scanned with a kVp of 100, and lowering the z-axis led to a reduction of DLP of 24% in the study subgroup.
In the subgroup of patients scanned without including the apices, one patient was recalled (0.5%) due to a perceived incompletely imaged abnormality at the right apex, according to Martins. On review by a consultant (senior) thoracic radiologist, the medical team decided the patient was inappropriately recalled.
"It was felt that the protocol could be safely implemented for routine use for the investigation of thromboembolic imaging as a dose-saving method. This is particularly useful in institutions with older scanners without iterative reconstruction," she concluded.