In what is thought to be the largest trial of its kind to date, U.S. and Italian researchers have found that an algorithm measuring blood flow through the coronary arteries based on data from CT images can prevent unnecessary catheterizations.
The study of nearly 600 patients imaged at 11 European centers using the Fractional Flow Reserve CT (FFRCT, HeartFlow) software showed almost three-fourths of patients with a scheduled invasive coronary angiography test had no significant blockages on angiography.
Conversely, just 12% of patients evaluated using an FFRCT-guided strategy went on to have an angiogram that showed no significant obstruction, concluded the study presented at the European Society of Cardiology (ESC 2015) in London and published concurrently in the European Heart Journal.
Coronary CT angiography (CTA) and fractional flow reserve by CTA is a safe and feasible alternative to angiography and was associated with a significantly lower rate of invasive angiography showing no obstructive coronary artery disease, wrote Dr. Pamela Douglas from Duke University Medical Center along with Dr. Gianluca Pontone from Centro Cardiologico Monzino in Milan and colleagues from 10 other European institutions (European Heart Journal, 1 September 2015).
In their multicenter prospective PLATFORM (Prospective longitudinal trial of FFRCT Outcome and Resource Impacts) trial, the authors aimed to determine if an FFRCT-guided strategy could reduce the use of invasive angiography procedures that turn out negative.
"The PLATFORM trial has shown in a subset of patients scheduled for catheterization according to standard care a 63% reduction in catheterization with a 32% reduction of overall cost," Pontone wrote in an email to AuntMinnieEurope.com.
Handling chest pain patients
The optimal evaluation of new-onset stable chest pain remains uncertain, the study team reported at ESC 2015. Two recent trials compared anatomic and functional strategies for workup, finding that CTA improved the care process. However, the modality also increased the number of invasive catheterizations and revascularizations without decreasing the number of cardiac events. Do catheterizations really need to increase?
FFRCT may address these limitations by providing both functional and anatomic data from CT angiography, the study team wrote. FFRCT uses computational fluid dynamics to model blood flow in the coronary arteries, and has been validated as accurate in smaller prior studies. Routine coronary CTA images are acquired at the point of care, and hen the data are transferred to the HeartFlow software for analysis, with data returned to the clinicians.
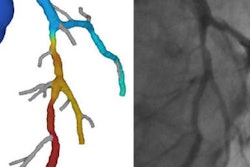
 FFRCT shows a hemodynamically significant lesion in the left anterior descending (LAD) artery. Images courtesy of lead author and ESC presenter Dr. Pamela Douglas.
FFRCT shows a hemodynamically significant lesion in the left anterior descending (LAD) artery. Images courtesy of lead author and ESC presenter Dr. Pamela Douglas.In the PLATFORM study, 584 patients (mean age 61, 40% female) with new onset chest pain were randomized at 11 sites globally to receive either usual testing (n = 287) or CTA plus FFRCT (n = 297). The clinical care team made all interpretation and care decisions. The primary endpoint of the study was determining the percentage of those with planned invasive coronary angiography studies who had no significant coronary disease at invasive angiography. The secondary endpoints included death, myocardial infarction, and unplanned revascularizations within 90 days. The patients mean probability of obstructive CAD was 49%.
Among those with planned invasive angiographies (193 FFRCT-guided, 187 with usual care) no obstructive coronary disease (luminal stenosis ≥ 50%) was found in 24 (12%) in the CTA/FFRCT arm and in 137 (73%) of the usual care group, yielding a difference in risk of significant CAD of 61%, p = 0.0001.
In fact, invasive angiography was cancelled in 61% of patients after receiving FFRCT results. Among patients with no planned invasive testing, the rates of finding no obstructive coronary after disease at invasive angiography were 13% for the CTA/FFRCT arm and 6% for the usual care arm (p = 0.20%).
In addition to reducing the rate of finding no invasive coronary disease at angiography from 73% to 12%, the study team reported similar results for all subgroups. Moreover, there was no difference in revascularization rates in patient with or without planned invasive angiography the authors wrote.
Finally, the use of FFRCT led to the cancellation of 61% of invasive coronary angiographies, and doubled the availability of functional data when interventions were performed, Douglas reported at ESC.
Among patients with planned invasive coronary angiography, the use of a combined anatomic and functional strategy employing CTA/FFRCT was "safe, and improved patient selection for invasive catheterization," Douglas and colleagues reported.
"This technique is ready for routine use to be accurate, and is associated with low radiation exposure as it does not require an additional scan," Pontone said. "More important, it does not require a specific background in the field of stress tests such as required for stress CT perfusion studies -- and this is a very appealing point for the radiology community."