Because of its high specificity and ability to differentiate between infection of the spine and other maladies, FDG-PET/CT should be the first option in suspected cases of spondylodiscitis, according to a Spanish study published online on 4 September in the European Journal of Nuclear Medicine and Molecular Imaging.
A team from the Barcelona Hospital Clinic, led by Dr. David Fuster from the nuclear medicine department, found that FDG-PET/CT outperformed the more commonly used MRI in the diagnosis of spondylodiscitis.
Spondylodiscitis is a combination of discitis, an inflammation of one or more intervertebral disk spaces, and spondylitis, an inflammation of one or more vertebrae. While MRI has been considered the most accurate modality for the early detection of spondylodiscitis, the modality cannot always be used due to the presence of other diseases.
"Furthermore," the authors wrote, "the role of MRI in postoperative infection of the spine remains controversial, because signal characteristics are not specific, making it more difficult to differentiate active infection from ongoing reparative and/or fibrotic tissue."
On the other hand, FDG-PET/CT may be useful to screen for spondylodiscitis in patients with infectious symptoms and may complement morphological MRI findings in patients with suspected spondylodiscitis.
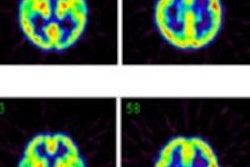
This prospective study included 14 men and 12 woman, with a mean age of 59 (± 17 years), who presented with back pain and clinical symptoms that indicated a spinal problem. Whole-body FDG-PET/CT scans were performed on all patients using a hybrid PET/CT scanner (Biograph, Siemens Healthcare). Patients fasted for six hours and were given 4.07 MBq/kg of FDG.
MRI of the spine was conducted on a 3-tesla scanner (Trio, Siemens), using several imaging techniques, including sagittal turbo SE T1-weighted and T2-weighted imaging and axial turbo T2-weighted imaging.
Two nuclear medicine specialists trained in infection imaging and two radiologists with training in infection with MRI interpreted the results. In addition, maximum standard uptake values (SUVmax) in the area suspected of infection and background SUVmean in a preserved area of the spine was used to help determine the presence of spondylodiscitis.
Finding spondylodiscitis
The results confirmed spondylodiscitis in 18 (69%) of the 26 patients and excluded the condition in the remaining eight individuals (31%). A further breakdown of the results found eight cases of staphylococcus aureus, four patients with mycobacterium tuberculosis, and two people with escherichia coli. The remaining four patients had other pathogens.
FDG-PET/CT also accurately discovered infection in the spine 15 (83%) of the 18 patients. The hybrid modality also showed no significant uptake of FDG in the spine, thus correctly excluding spondylodiscitis in seven (87%) of the eight noninfected patients.
The SUVmean for infected patients was 6.522, compared with 3.675 for noninfected patients, achieving a statistically significant difference between the two measures.
| Results for detection of spondylodiscitis | ||
| FDG-PET/CT | MRI | |
| Sensitivity | 83% | 94% |
| Specificity | 88% | 38% |
| Positive predictive value | 94% | 77% |
| Negative predictive value | 70% | 75% |
| Accuracy | 84% | 81% |
Given FDG-PET/CT's results with sensitivity, specificity, and an "outstanding" positive predictive value, Fuster and colleagues described these numbers as "encouraging and make FDG-PET/CT a robust technique for differentiating spondylodiscitis from other processes."
The study also found only one false-positive with FDG-PET/CT in cases of postfracture changes, compared with MRI, which had false-positive results with five patients. Three of those five people were diagnosed with postfracture changes and the other two people had spondyloarthropathy.
MRI also registered one false-negative, while FDG-PET/CT showed no significant uptake in three (19%) of the 18 patients with a final diagnosis of spondylodiscitis.
"In this series, the addition of FDG-PET/CT helped diagnose infection in the patient false-negative on MRI," the authors wrote. "Thus the combination of FDG-PET/CT and MRI detected the infection in 100% of patients with spondylodiscitis, which is the most relevant finding, as a delayed diagnosis can result in potentially serious complications."
There may still be situations in which the diagnosis of spondylodiscitis is difficult as in the presence of vertebral fractures where imaging procedures may show false-positive findings as was seen in this series with FDG-PET/CT in one patient and with MRI in all three patients.
FDG-PET/CT should be considered in the evaluation of suspected spondylodiscitis and may be of most use in patients in whom MRI is suggestive of infection but no soft-tissue involvement is present, avoiding false-positive results for infection of the spine, they concluded.
Quantification with SUVmax, especially with correction using the background SUVmean, discriminated infection of the spine from other processes in this series. The results indicate that FDG-PET/CT may become the imaging procedure of choice in the diagnosis of infective spondylodiscitis.