Knowledge and experience gained by elite sports medicine centers can be applied to a more general setting, according to Dr. Patricia Cunningham.
European Society of Radiology (ESR): Sports imaging is the main theme of International Day of Radiology (IDoR) 2019. In most countries, this is not a specialty in itself, but a focus within musculoskeletal radiology (MSK). In your country, is there a special focus on sports imaging within radiology training or special courses for interested radiologists?
 Dr. Patricia Cunningham.
Dr. Patricia Cunningham.Cunningham: In Ireland, sports imaging is part of MSK radiology and is performed mostly by radiologists with MSK training. There is no special focus on sports imaging for trainee radiologists, but they would be exposed to common sporting injuries during their MSK training/modules. There are no dedicated training courses for radiologists interested in sports imaging, but most MSK radiologists attend international meetings and courses to learn or maintain skills.
Please describe your regular working environment (hospital, private practice). Does sports-related imaging take up all, most, or only part of your regular work schedule?
I work in two teaching public hospitals, neither of which have radiology trainees, but they do have trainees in other specialties. In Ireland, public hospitals have some private practice attached, and I work in this sector as well. I believe MSK imaging and procedures, including sports, take up approximately 60% of my clinical work.
Based on your experience, which sports produce the most injuries that require medical imaging? Have you seen any changes in this regard during your career? What areas/types of injuries provide the greatest challenge to radiologists?
The most commonly played sports in Ireland are football, rugby, and our national games of hurling and Gaelic football. These generate most of the injuries that require imaging. The injuries do vary among the sports; for example, hand and finger injuries are very common in hurling as this is played with a hurley stick; often radiographs are all that are required.
Gaelic football has similar injuries to football with groin, hamstring, and knee injuries being common. Besides, as Gaelic football allows catching of the ball, there are shoulder injuries similar to those in rugby. In the last decade or so, the change I have noticed most is the pattern of muscle injuries in the pelvis/thighs with fewer hamstring injuries and more groin injuries.
Muscle injuries, I think, are the most challenging for several reasons. The extent of the injury is often over- or underdiagnosed clinically before imaging occurs, and this can affect the clinical team and the player in terms of mental and physical response. The return-to-play time has become such an important feature of imaging that it adds extra pressure to the reporting radiologist, potentially causing some conflict with other members of the medical management team. Pressure can also come from players themselves in terms of wanting to return as early as possible, which may cause some tension or disagreement between the radiologist and the sports physician/team doctor.
 Coronal proton density-weighted MR image shows femoroacetabular impingement of the cam type. "Bump" from bone formation at the femoral head/neck junction (white arrow) with full-thickness articular cartilage defects of acetabulum (black arrow) and labral tear (red arrow). All images courtesy of Dr. Patricia Cunningham.
Coronal proton density-weighted MR image shows femoroacetabular impingement of the cam type. "Bump" from bone formation at the femoral head/neck junction (white arrow) with full-thickness articular cartilage defects of acetabulum (black arrow) and labral tear (red arrow). All images courtesy of Dr. Patricia Cunningham.Please give a detailed overview of the sports injuries with which you are most familiar and their respective modalities.
In my practice, we see a large amount of knee injuries (meniscal, cruciate, and medial collateral ligament) -- ankle injuries, predominantly ligaments, shoulders (dislocations with sequelae of same), hand injuries (particularly fractures in hurling and ulnar collateral ligament injuries), and groin pain (osteitis pubis, adductor/gracilis/rectus abdominis injuries, labral tears).
MRI is our test of choice for nearly all sports injuries, apart from obvious fractures and hand injuries. All knee, shoulder, hip, groin, and muscle injuries are evaluated with MRI. Shoulder and hip MR arthrography are reserved for those who have indeterminate noncontrast MRI for evaluation of labral and cartilage injuries or who have a high level of suspicion for these injuries from the outset. Ultrasound is often the first test for tendon injuries, such as Achilles, peroneal, and wrist tendons, with MRI reserved for more detailed analysis as necessary.
What diseases associated with sporting activity can be detected with imaging? Can you provide examples?
It is not uncommon to image players for a specific injury and find incidental pathology. This is similar to the general population and not really specific to sports players. The age profile of the individuals commonly imaged also is relatively young, making other diseases less likely. However, with increased focus on health and fitness in the community at large, we are seeing more older people for sports imaging (especially runners) who are more likely to have an incidental finding. On occasion, someone may present with back or pelvic pain presumed to be due to sporting injury but may be inflammatory arthropathy, as this would be commonly seen/diagnosed in young adults. Imaging performed for symptoms thought to be related to a sports injury rarely diagnoses a tumor.
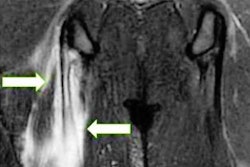
 Coronal short-tau inversion-recovery (STIR) MR image shows a right accessory cleft sign (red arrow) with parasymphyseal marrow edema (black arrow) compatible with adductor/gracilis dysfunction and osteitis pubis.
Coronal short-tau inversion-recovery (STIR) MR image shows a right accessory cleft sign (red arrow) with parasymphyseal marrow edema (black arrow) compatible with adductor/gracilis dysfunction and osteitis pubis.Radiologists are part of a team; for sports imaging, this likely consists of surgeons, orthopedists, cardiologists, and/or neurologists. How would you define the role of the radiologist within this team, and how would you describe the cooperation among radiologists, surgeons, and other physicians?
Radiologists are an integral part of the multidisciplinary team managing sports injuries. I would say the radiologist works closest with the sports physician/team doctor, and most decisions would be made in this realm. I see major roles for the radiologist as follows: confirming an accurate diagnosis by the most appropriate imaging modality; helping to inform decisions regarding management, including return to play; performing certain procedures/injections; and, to a lesser extent, helping with preparticipating assessments.
Generally, each team member works well for the best outcome of the player, but occasionally there can be conflict, particularly in relation to return-to-play time as mentioned earlier. Many sports physicians are quite skilled in using ultrasound and interpreting MRI, and this sometimes leads to discussion/dispute when there is a difference of opinion with the radiologist.
The role of the radiologist in determining diagnoses with sports imaging is obvious. How much involvement is there regarding treatment and follow-up?
As I mentioned above, I feel the role of the radiologist incorporates performing certain procedures/injections and evaluating return-to-play time. The latter, in particular, is a growing area with healing being evaluated using imaging during the course of rehabilitation rather than just initially or at the end.
Radiology is effective in identifying and treating sports-related injuries and diseases, but can it also be used to prevent them? Can the information provided by medical imaging be used to enhance the performance of athletes?
I do not have much experience with screening and preassessment. In principle, it is a good idea, but with existing limited resources it would be difficult to implement. Imaging would be helpful in diagnosing cases of tendinopathy/partial tendon to help prevent complete tears, which would, for example, have significantly higher morbidity. I think a very important role is played by our cardiac colleagues in trying to identify those at risk of sudden cardiac events during sport.
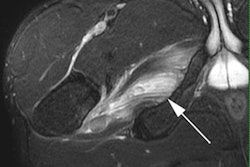
 Coronal STIR MR image shows a left accessory cleft sign (red arrow) with parasymphyseal marrow edema (black arrow) compatible with adductor/gracilis dysfunction and osteitis pubis.
Coronal STIR MR image shows a left accessory cleft sign (red arrow) with parasymphyseal marrow edema (black arrow) compatible with adductor/gracilis dysfunction and osteitis pubis.Many elite sports centers use cutting-edge medical imaging equipment and attract talented radiologists to operate it. Are you involved with such centers? How can the knowledge acquired in this setting be used to benefit all patients?
I do not work in a specialist sports center, but many of the injuries that are seen in amateur and "weekend warrior" type sports are the same as those in professional athletes in more elite centers. All knowledge and experience gained in these centers can be applied to a more general setting. The increased number of injuries seen in a specialist center allows expertise and skill to develop quickly, and this can then be disseminated more widely.
The demand for imaging studies has been rising steadily over the past decades, placing strain on healthcare budgets. Has the demand also increased in sports medicine? What can be done to better justify imaging requests and make the most of available resources?
In my practice, the majority of sports imaging costs are covered by insurance with the sports clubs as long as the injury took place during club activity. This takes the burden away from the individual. However, in Ireland as elsewhere, there are limited resources, especially in terms of MRI -- the modality that is relied upon most in sports imaging. Like all imaging, good clinical assessment and close cooperation with the other members of the medical management team can help optimize the resources available.
Athletes are more prone to injuries that require medical imaging. How much greater is their risk of developing diseases related to frequent exposure to radiation, and what can be done to limit the negative effects from overexposure?
The risk from exposure to radiation from medical imaging is very small. As I alluded to earlier, most sports imaging relies on MRI and ultrasound, which have no ionizing radiation. The small doses of radiation used in image-guided procedures and radiographs do not pose a significant risk, and, of course, all precautions are taken (as with everybody) to keep the dose as low as reasonably achievable.
Do you actively practice sports yourself and, if yes, does this help you in your daily work as an MSK radiologist?
I used to participate more when I was younger, but I have a keen interest in sport generally. I think this does help in terms of understanding injury mechanics and makes me more empathetic with the players.
Dr. Patricia Cunningham, MBBChBAO, MMedSci, MSC, FFR RCSI, is a consultant radiologist at Our Lady of Lourdes Hospital in Drogheda and Our Lady's Hospital in Navan. She is also the vice dean of the Faculty of Radiologists in Ireland and is chair of its Professional Competence Scheme and Quality Improvement Committee. She has served on the MSK subcommittee of ECR 2011-2013 and the RSNA Education Awards Committee (MSK section) 2017-2019. She has given invited lectures, tutorials, and refresher courses, as well as moderated at many national and international meetings, including ECR, European Society of Musculoskeletal Radiology, and RSNA. Dr. Cunningham has been an associate editor of Radiology since January 2013 and acts as a reviewer for Radiology and the Journal of Magnetic Resonance Imaging.
Editor's note: This is one of a series of interviews with 40 MSK and sports imaging experts from Europe, North America, Latin America, Asia, Australia, and South Africa. These interviews are available for free on the IDoR website.
Copyright © 2019 European Society of Radiology