Radiologists are always on the lookout for the latest and greatest technology, and this is particularly true in breast imaging, because the primary modality, mammography, is not exactly perfect. Rapid progress in both CT and MRI are being made in this field.
"There is a general consensus that the sensitivity and specificity of screening mammography is unsatisfactorily low," Dr. Willi Kalender, PhD, chairman of the Institute of Medical Physics at the University of Erlangen in Germany, told ECR Today. "MRI offers much higher values but lacks imaging of microcalcifications, is more costly, and [is] time-consuming."
As an alternative, he suggests dedicated breast CT, first described in detail in 2012. The goal of breast CT is to offer high-resolution CT imaging at a very low dose and increased sensitivity and specificity. CT can offer superposition-free imaging with a very high spatial resolution of 100 µm or better in all three spatial dimensions, dose levels low enough to conform with mammographic screening regulations, dynamic imaging with contrast medium application when indicated, and integrated biopsy capabilities, he explained.
 A breast CT scanner with the patient in prone position with one breast being imaged at a time (typically 10 seconds or less) and without compression. Image courtesy of Dr. Willi Kalender.
A breast CT scanner with the patient in prone position with one breast being imaged at a time (typically 10 seconds or less) and without compression. Image courtesy of Dr. Willi Kalender."The overall goal is a 'one-stop shopping device' for breast patients allowing for plain scans, for contrast-enhanced studies, and for support of interventions," Kalender said. "This will potentially replace the lengthy stepwise procedure (mammography, ultrasound, MRI, biopsy), which means consecutive with long wait times."
The first two breast CT scanners, also called demonstrators, are in preparation for clinical installation at the university hospitals in Aachen and Erlangen. Clinical testing is due to start around the middle of this year.
Breast MRI is also progressing. Unenhanced MRI may simplify the approach to breast MRI by omitting costs, time effort, and potential side effects related to contrast agents, including circulation-related effects, allergies, nephrogenic systemic fibrosis, according to Dr. Pascal Baltzer, associate professor in the radiology department at the Medical University of Vienna. An imaging protocol using unenhanced MRI only -- as in diffusion-weighted imaging (DWI) together with T2-weighted anatomical images -- would require about five to 10 minutes of magnet time, thus allowing the examination of at least six patients per hour, he said. Also, reduced costs could broaden the availability of breast MRI.
![A full examination at 3 tesla. A, B, and C: Precontrast T1-weighted imaging, early and delayed postcontrast scans depicting a mass (invasive ductal carcinoma, arrow) and associated clapped segmental nonmass enhancement (dashed arrow, ductal carcinoma in situ [DCIS]). D: The SI-time curve of the mass, indicating a malignant lesion by washout type 3 curve. E: The DWI image where the cancer lesions can be seen hyperintense similar to contrast-enhanced images. F: The apparent diffusion coeficient (ADC) map where the tumors are indicated by low signal intensity corresponding to typical restricted diffusion. Note that the signal of the invasive cancer is lower than that of the DCIS, confirming the ability of DWI to demonstrate quantitative differences in tissue microstructure not only able to diagnose cancer but also to differentiate invasive from noninvasive cancer. Images courtesy of Dr. Pascal Baltzer.](https://img.auntminnieeurope.com/files/base/smg/all/image/2015/03/ame.2015_03_04_22_11_00_218_2015_03_05_enhanced_MRI1.png?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) A full examination at 3 tesla. A, B, and C: Precontrast T1-weighted imaging, early and delayed postcontrast scans depicting a mass (invasive ductal carcinoma, arrow) and associated clapped segmental nonmass enhancement (dashed arrow, ductal carcinoma in situ [DCIS]). D: The SI-time curve of the mass, indicating a malignant lesion by washout type 3 curve. E: The DWI image where the cancer lesions can be seen hyperintense similar to contrast-enhanced images. F: The apparent diffusion coeficient (ADC) map where the tumors are indicated by low signal intensity corresponding to typical restricted diffusion. Note that the signal of the invasive cancer is lower than that of the DCIS, confirming the ability of DWI to demonstrate quantitative differences in tissue microstructure not only able to diagnose cancer but also to differentiate invasive from noninvasive cancer. Images courtesy of Dr. Pascal Baltzer.
A full examination at 3 tesla. A, B, and C: Precontrast T1-weighted imaging, early and delayed postcontrast scans depicting a mass (invasive ductal carcinoma, arrow) and associated clapped segmental nonmass enhancement (dashed arrow, ductal carcinoma in situ [DCIS]). D: The SI-time curve of the mass, indicating a malignant lesion by washout type 3 curve. E: The DWI image where the cancer lesions can be seen hyperintense similar to contrast-enhanced images. F: The apparent diffusion coeficient (ADC) map where the tumors are indicated by low signal intensity corresponding to typical restricted diffusion. Note that the signal of the invasive cancer is lower than that of the DCIS, confirming the ability of DWI to demonstrate quantitative differences in tissue microstructure not only able to diagnose cancer but also to differentiate invasive from noninvasive cancer. Images courtesy of Dr. Pascal Baltzer."The issue is the broad variability of DWI imaging results," he noted. "Although several initial studies have demonstrated a similar performance of unenhanced breast MRI compared with breast MRI, these studies did not answer how good unenhanced MRI is for specific indications (such as high-risk screening, etc.). Furthermore, potential pitfalls such as mastopathic changes, small and nonmass lesions have not been closely investigated."
At the moment, contrast-enhanced breast MRI is the standard of care, and this won't change until more research has covered the field of unenhanced breast MRI. "However, we have to keep in mind that leading experts in prostate MRI openly discuss whether contrast agent application is really necessary," he said.
Unenhanced breast MRI could be used in nearly all fields of breast MRI, given an appropriate DWI technique, he remarked. However, typical pitfalls include chronic inflammatory conditions such as regularly seen in postsurgical conditions.
"As a matter of fact, I would not primarily recommend the use of enhanced MRI in the differentiation between scar and cancer recurrence," he stated. "Even simple MRI techniques might help in the differentiation of multiple mass lesions or cancer staging, or, more generally, in the characterization of a definite anatomical area of uncertainty."
At today's special focus session, Baltzer promises to give an overview of what's possible with unenhanced breast MRI. He said he always tries to be critical, will provide an evidence-based overview on possibilities, limitations, and developments in unenhanced breast MRI.
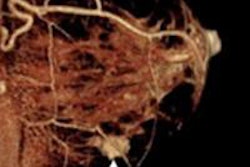
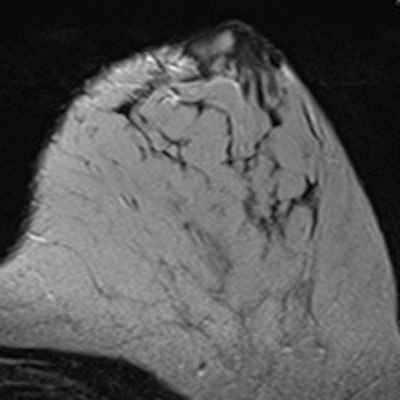
 A rim-enhancing mass on contrast-enhanced subtraction. The unenhanced scan shows a high signal intensity of the whole lesion on the diffusion-weighted image, higher than normal cancer. It corresponds to a restricted diffusion of the whole lesion and intermediate high signal intensity on the T2-weighted turbo spin-echo scan. The finding is typical for an abscess: If this were a cancer, the central necrosis should not show restricted diffusion or at least the restricted diffusion should correspond with the enhancement. It is a nice example how DWI (and subsequently unenhanced MRI) may lead to a better diagnosis compared with contrast-enhanced imaging. Images courtesy of Dr. Pascal Baltzer.
A rim-enhancing mass on contrast-enhanced subtraction. The unenhanced scan shows a high signal intensity of the whole lesion on the diffusion-weighted image, higher than normal cancer. It corresponds to a restricted diffusion of the whole lesion and intermediate high signal intensity on the T2-weighted turbo spin-echo scan. The finding is typical for an abscess: If this were a cancer, the central necrosis should not show restricted diffusion or at least the restricted diffusion should correspond with the enhancement. It is a nice example how DWI (and subsequently unenhanced MRI) may lead to a better diagnosis compared with contrast-enhanced imaging. Images courtesy of Dr. Pascal Baltzer."Breast imaging is rapidly evolving as a dedicated imaging modality," said session moderator Dr. Marc Lobbes, PhD, from the radiology department at Maastricht University Medical Centre in the Netherlands. "Many imaging tools currently exist, from basic mammography, ultrasound, and MRI, to elastography, digital breast tomosynthesis, contrast-enhanced spectral mammography, state-of-art MRI sequences, and PET/MRI, to name but a few."
He plans to provide an overview for both dedicated and general radiologists of the current most promising developments, including contrast-enhanced mammography, also called contrast-enhanced spectral mammography (CESM), which became commercially available in 2011. It uses an iodine-based contrast agent and a dual-energy technique to increase the diagnostic accuracy of mammography.
"In recent years, many studies have shown that CESM is consistently superior to full-field digital mammography [FFDM] in breast cancer detection and able to achieve results similar to breast MRI, which is still considered to be the most accurate breast cancer detection modality," Lobbes noted.
 An example of a complete contrast-enhanced spectral mammography (CESM) exam, which consists of a normal mammogram (left), followed by a high-energy image (middle, which is not for diagnostic purposes). These two images are postprocessed to generate the recombined image (right), which is showing areas of enhancement. The arrows indicate the breast cancer. In a CESM exam, only the left and right image are presented to the radiologist. Images courtesy of Dr. Marc Lobbes.
An example of a complete contrast-enhanced spectral mammography (CESM) exam, which consists of a normal mammogram (left), followed by a high-energy image (middle, which is not for diagnostic purposes). These two images are postprocessed to generate the recombined image (right), which is showing areas of enhancement. The arrows indicate the breast cancer. In a CESM exam, only the left and right image are presented to the radiologist. Images courtesy of Dr. Marc Lobbes.CESM could easily be implemented in everyday clinical practice, but there are some disadvantages, such as the use of iodine-based contrast agents and the 80% increase in radiation dose. Also, CESM doesn't have proper indications, he added.
"Although it is superior to FFDM and the principle is similar to that of breast MRI, proper indications are still lacking," he stated. "Nonetheless, many studies are currently ongoing to clarify the strengths and weaknesses of CESM, so it is safe to assume that more knowledge on CESM indications will be gathered in the next few years."
Originally published in ECR Today on 5 March 2015.
Copyright © 2015 European Society of Radiology