Image guidance during radiotherapy can reduce target positioning errors and increase treatment efficacy. MRI is an excellent candidate for such a task, with its superior soft-tissue contrast providing a clear view of both tumor tissue and organs at risk. However, magnetic field inhomogeneities arising from patient anatomy can lead to image distortion.
A research team at the University Medical Center Utrecht in the Netherlands has developed a method for correcting such distortions, and demonstrated its use with phantom and anatomical MR images. The proposed scheme requires just a few milliseconds of processing time, making it fast enough for near-real-time feedback during irradiation (Physics in Medicine and Biology, January 7, 2011, Vol. 56:1, pp. 289-298).
"With MRI guidance, one truly sees the target to be hit. Having good soft-tissue contrast enables direct and real-time identification of the treatment volume during each therapy session," PhD researcher Sjoerd Crijns told medicalphysicsweb. "But image distortion is a problem in MRI applications where high geometric fidelity is desired. MRI for radiotherapy is demanding, since distortions in the (pretreatment) images lead to incorrect treatment plans and hence missing the tumor."
Pixel tracking
 |
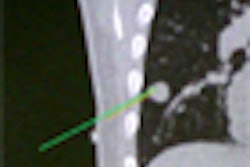
| CT of the head-and-neck area (left) and the magnetic field distribution in ppm of the nominal value (right). |
To test the validity of this correction procedure, the researchers examined a water-filled phantom containing a regular 2D plastic grid. The phantom was imaged using a GRE sequence with a low gradient strength (0.93 mTm-1), which leads to large image deformations.
"We acquired images with low gradient strength to illustrate the large deformations that may occur and show that we are able to correct the distortions even in those cases," Crijns explained. "This proves the robustness of our implementation."
Crijns and colleagues determined the locations of the central 64 grid points before and after correction, and compared these to their expected locations, as defined from a CT image of the phantom. The average difference between the MRI-obtained grid point locations and their real coordinates was 0.65 mm before correction. After correction, this was reduced to 0.30 mm. The maximum displacement of 2.9 mm seen before correction was reduced to 0.63 mm after correction.
 |
| MR images of the phantom before and after correction, the measured field map used for correction, and a CT image. |
The team then validated the scheme for an in vivo application, using it to extract body contours for prostate treatment planning. Here, a spin-echo MR image was acquired from a healthy volunteer, using a readout gradient of 1.0 mTm-1 and an acquisition time of 76.8 sec. For comparison, a second image was obtained using the same imaging parameters but a higher readout gradient of 15.0 mTm-1. The magnetic field map was acquired using a GRE sequence.
The displacement map showed distortions in the high-gradient image to be within 0.5 mm. This image was therefore deemed suitable as a ground truth for comparison with the low-gradient image. Before correction, distortions in the low-gradient image were as large as 6 mm, with a similar displacement seen in extracted pelvic contours. After correction, the differences as compared to the ground truth contour were reduced to 2 mm (one voxel) or less.
Implementation
Following field map acquisition, the corrected images can be created in 8 msec or less, with an accuracy comparable to previous correction methods that take far longer to process. The Utrecht scheme can thus be considered a viable tool for enabling MR-guided radiotherapy with online MRI-based plan adaptations.
The researchers note that the image correction scheme could prove particularly valuable for imaging small radiotherapy targets within heterogeneous anatomies. In head-and-neck cases, for example, where tissue/air/bone transitions cause large field inhomogeneity, MR images recorded with a gradient strength of 1 mTm-1 can be distorted by as much as 9 mm.
Another potential application is MR-guided proton therapy, not yet available but an attractive concept. Image distortion can seriously impact proton therapy guidance, as even small inaccuracies in depth targeting can lead to serious dosimetric errors. Corrected MR images could provide online updates of patient contours and geometric information on internal structures.
The Utrecht team is now investigating image-corrected MRI-guidance for radiotherapy of moving targets. This is a more complex problem as breathing motion may lead to inaccurate magnetic field maps (due to inaccurate pixel-to-pixel correspondence between the two images used for field mapping).
"We are also working on an imaging sequence that is insensitive to magnetic field inhomogeneities to prevent the whole problem from occurring," said Crijns.
By Tami Freeman
Medicalphysicsweb editor
February 4, 2011
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community website covering fundamental research and emerging technologies in medical imaging and radiation therapy.